I'm not quite sure if it is my generation or basic human need, but I have trouble dealing with criticism.
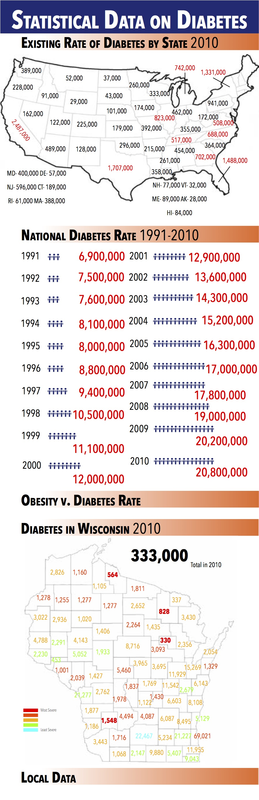
Last week we presented our graphics to the Daria's class in an attempt to get some feedback. Mine could've gone better. It worked, but it combined my fear of public speaking with my fear of presenting things I've made. It was sort of like the perfect storm.
I took the criticisms they had and worked it into my project. I'm currently busy adding a new element to my graphic as well. The critiques that Daria's class gave were right on par, and overall they helped me grow as a graphic artist - something I don't consider myself to be.
This info graphic has started to challenge me. I thought I was the best, and I thought my graphic was very good - but that's not the case as I'm starting to realize.
The worst part is trying to find a way to do everything when you have a lot to do.
I'm not going to say I'm not looking forward to this week because that isn't true. I just think I'm a little overbooked.
Last week we presented our graphics to the Daria's class in an attempt to get some feedback. Mine could've gone better. It worked, but it combined my fear of public speaking with my fear of presenting things I've made. It was sort of like the perfect storm.
I took the criticisms they had and worked it into my project. I'm currently busy adding a new element to my graphic as well. The critiques that Daria's class gave were right on par, and overall they helped me grow as a graphic artist - something I don't consider myself to be.
This info graphic has started to challenge me. I thought I was the best, and I thought my graphic was very good - but that's not the case as I'm starting to realize.
The worst part is trying to find a way to do everything when you have a lot to do.
I'm not going to say I'm not looking forward to this week because that isn't true. I just think I'm a little overbooked.


 RSS Feed
RSS Feed